Analysis and reporting on politics and culture in America. Home to Sarah Longwell, Tim Miller, Bill Kristol, JVL, Sam Stein, and more.
No partisan loyalties. No tribal prejudices.
Every week I highlight three newsletters that are worth your time.
If you find value in this project, do two things for me: (1) Hit the like button, and (2) Share this with someone.
Most of what we do in Bulwark+ is only for our members, but this email will always be open to everyone. To get it each week, sign up for free here. (Just choose the free option at the bottom.)
Statistics are tricky! David Epstein is here to explain what it means to have a test that is “95 percent accurate”:
Pretend You’re A Doctor…
…and here’s the scenario:
You’re using a new test for Disease X, which afflicts 1 out of every 1,000 adults. The new test has perfect “sensitivity,” i.e. it detects every single true positive case of Disease X. It also has a false positive rate of 5%. Your last patient doesn’t have obvious symptoms, but you just got their positive test result. What is the chance that they actually have Disease X?
For a 2014 study, the above question was given to doctors and med students. The most common answer they gave was that the patient has a 95% chance of actually having the disease. The correct answer, however, is that there is only about a 2% chance that the patient actually has the disease — 1.96% to be exact.
Let’s say we randomly test 10,000 people for Disease X; remember, only 1 in 1,000 people get Disease X. If our sample is representative of the general public, 10 of those 10,000 will have Disease X. Because the test has perfect sensitivity, all 10 of those people will get a true positive result.
But given the 5% false positive rate, 5 out of every 100 people tested in the entire group will get a false positive. That’s 500 false positives in 10,000 tests.
So in our batch of 10,000 test results, there are 10 true positives, and 500 false positives — 510 positives overall. Thus, the chance of a patient who tests positive actually having the disease is 10/510, or 1.96%. . . .
The more rare the condition . . . the lower the false positive rate must be in order for false positives not to outnumber true positives. This is one reason why guidelines for prostate and breast cancer suggest that screening for most people should not begin until at least middle age. As people age, the prevalence of those cancers in the population increases, and so does the probability that a positive test is a true positive. In other words, the ratio of true positives to false positives increases as an illness gets more common, making the screening test a more reliable tool. . . .
You really have to know how common an illness is in the first place (its “base rate”) in order to know the test’s “positive predictive value,” or how definitive a positive result really is.
Katelyn Jetelina does epidemiology in a way that’s accessible and helpful. I wish everyone in America would read this post on masks:
[T]he authors pooled 72 studies to assess how different public health mitigation measures (like masks, socially distancing, handwashing, etc.) impacted COVID19 infection. They found that some public health measures don’t really work. But, mask wearing reduced COVID19 infection by 53%. (For the record, this isn’t the only publication that shows masks work. For example, here are three studies that show they work well in schools.)
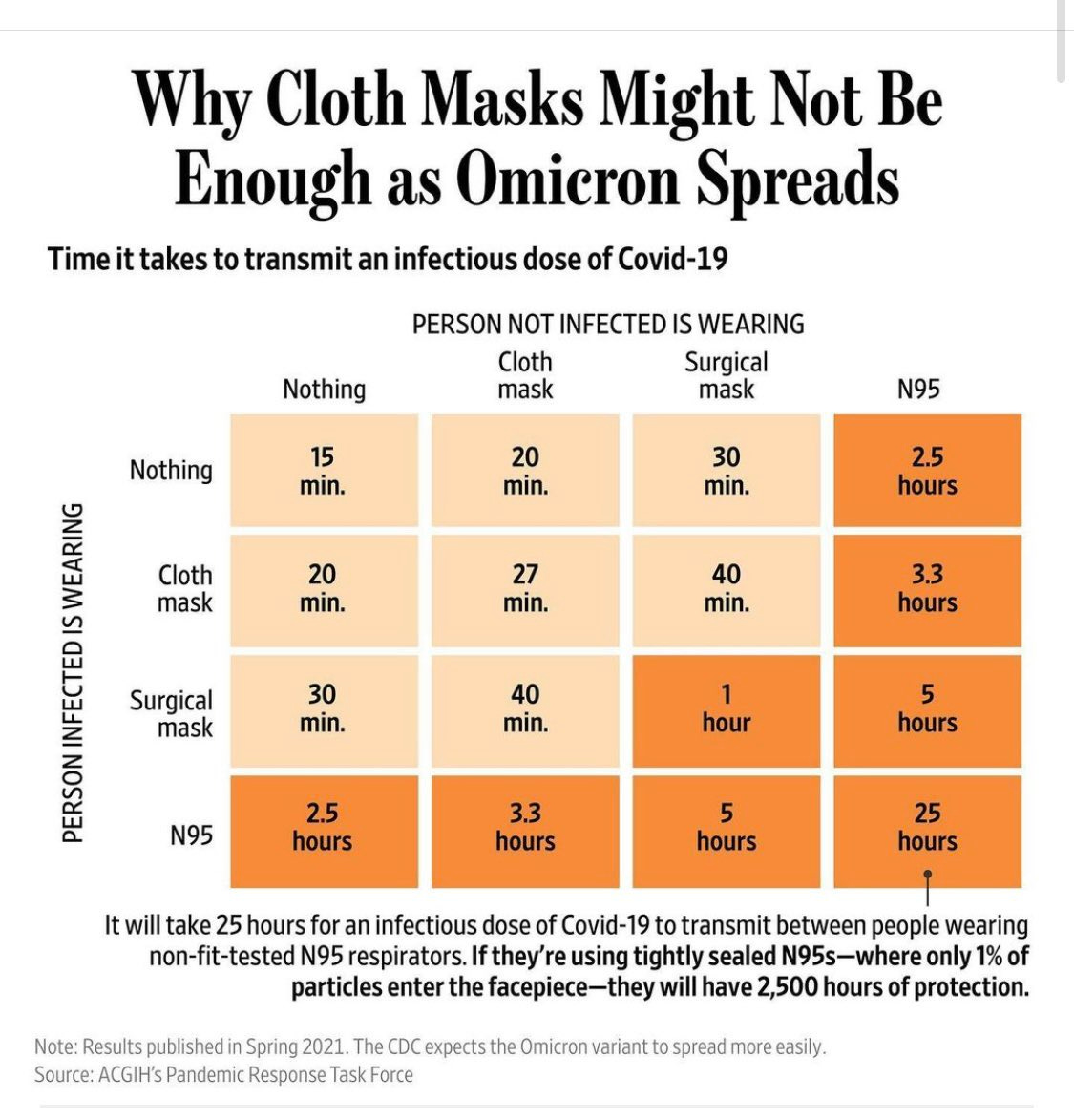
Mask effectiveness is certainly dependent on the type of mask, though. This is why a layered approach (vaccine, mask, ventilation, testing) is crucial, especially in light of Omicron. The Wall Street Journal published a great graphic earlier this week comparing the protection of different types of masks:
(WSJ)
For those of you looking for masks, I’m a big fan of Aaron Collins who calls himself the “Mask Nerd”. He is mechanical engineer with a background in aerosol science. Since the beginning of the pandemic he has been testing, documenting, and reviewing the best masks he could find (in his free time). He has a YouTube channel and an incredible database. I will say, though, the adult database is overwhelming. The kids database is much better. His video on masks for kids under 12 was fantastic, too.
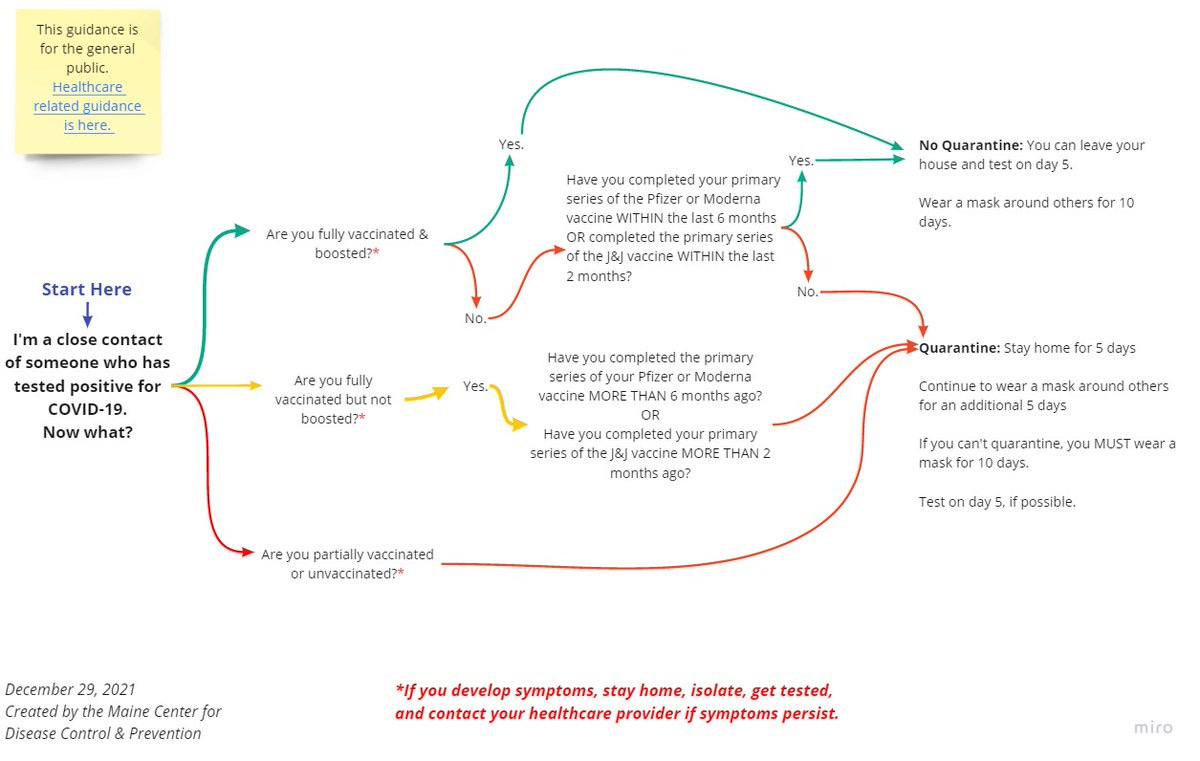
And she also has a helpful guide for what to do if you’ve had a close contact with COVID:
The CDC guidance for isolation is beyond confusing. And I’m incredibly disappointed in their lack (or complete disregard) of scientific communication. I was going to put together a flow chart about what the guidance actually says. But, I found that the Maine CDC put together a fantastic one already:
Here is what you need to do if you’re in close contact of someone who has tested positive for COVID19:
I never do this, but we have a weekly livestream that’s only for Bulwark+ members and this week I’ve unlocked it so that you can go back and watch the episode. It was a pretty great show. We talked about January 6. (And Hamilton.) Charlie Sykes and Amanda Carpenter argued about whether or not Mike Pence is a hero. And I referred to a certain formerly-important Good Republican as Shorty McHotpants.
The reason I’ve opened up Thursday Night Bulwark is because this week we wrapped up our third year of operation and we’re growing and expanding and I want you to be a part of it.
Here’s the thing: The Bulwark is a mission-focused operation. We’re here to protect democracy and build a better public square. We’re not doing this to get rich. That’s why we put most of what we do out into the world and don’t keep it locked behind a paywall. Because you change the world by being in the world.
But we do keep some things just for members of Bulwark+, because they’re the people supporting the mission and building this community with us. Thursday Night Bulwark is one of those members-only things. My daily newsletter is another. So’s the Secret Podcast. (Which I can’t even tell you about. Sorry.)
Today I’m inviting you to join us. You don’t have to, obviously. You’ll still always get this Saturday Newsletter of Newsletters. And you’ll still be able to read and listen to most of what we do.
But I don’t view Bulwark+ as a fee-for-service. And most of our members don’t, either. It’s planting a flag and helping to build something better.
Anyway, I hope you’ll think about joining. And to help you along, I’ve got a one-time offer for you to get a free 30-day membership.













{kind=link}